Radiographic Positioning of the Knee Patella Views

This article for the Radiologic Technologist (X-Ray Tech) discusses radiographic positioning of the knee for patella views.
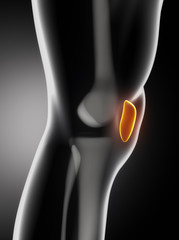
Patella PA
Purpose and Structures Shown To show the patella in PA projection. This view shows greater detail in the patella due to the decreased OID (object to image receptor distance).
Position of patient Prone position with the legs extended. Place one sandbag under the thigh and another under the leg to relieve pressure on the patella, if needed.
Position of part Center the IR to the patella. Adjust the leg so that the patella is parallel with the plane of the IR. This usually requires the heel to be rotated 5 to 10 degrees laterally.
Central ray Perpendicular to the IR and the midpopliteal area, exiting at the patella. Collimate closely to the patellar area.
Technical factors Visualization of soft tissues and sharp trabecular markings in the distal femur as well as a clear outline of the patella indicate optimal exposure without motion. Adequate penetration is necessary to see the patella through the superimposing femur. No rotation should be present.
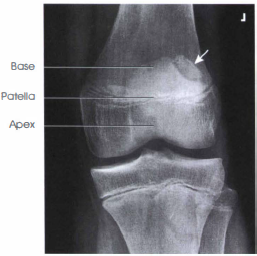
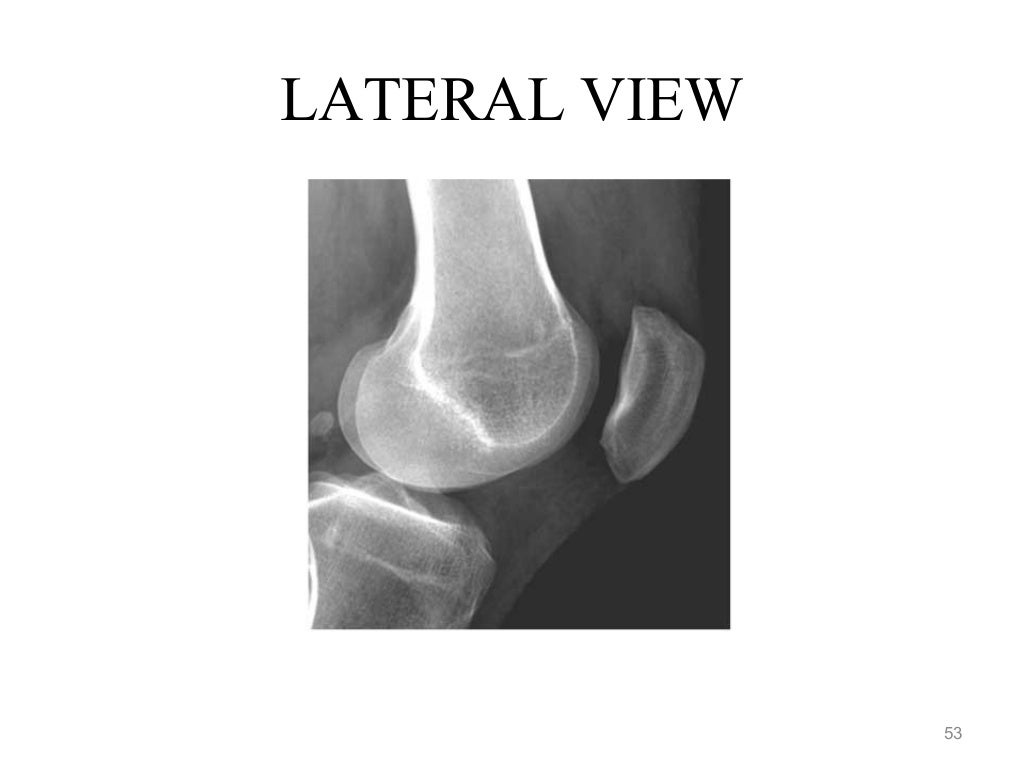
Patella Lateral
Purpose and Structures Shown Patella in lateral profile and patellofemoral joint space.
Position of patient Lateral recumbent position.

Position of part Ask the patient to turn onto the affected hip. A sandbag may be placed under the ankle for support. Flex the affected knee about 5-10 degrees. Increasing flexion reduces the patellofemoral joint space. Femoral epicondyles should be perpendicular to the IR.
Central ray Perpendicular to the IR, entering the knee at the patella. Collimate closely to the patellar area.
Insall-Salvati Ratio This is a ratio that is used to evaluate the position of the patella. It is the ratio of the longest diagonal length of the patella to the length of the patellar tendon on a lateral radiograph. This measurement is relatively independent of the degree of knee flexion. A ratio of less than 0.8 is indicative of patella alta (high-riding patella).
Insall-Salvati ratio patella

Insall-Salvati ratio measurement to assess the position of the patella.
Patella PA Oblique Lateral Rotation
Purpose and Structures Shown Medial margin of the patella superimposed over the femur and also the lateral aspect of patella free of the femur.

Position of patient Prone position.
Position of part Flex the knee 5-10 degrees. Externally (laterally) rotate the knee 45 -55 degrees from prone position.
Central ray Perpendicular to the IR, exiting the palpated patella. When the patella is being imaged, collimation should be to the mid-knee area.
Patella PA Oblique Medial Rotation
Purpose and Structures Shown Majority of the medial patella without the femur.

Position of patient Prone position.
Position of part Flex the patient’s knee about 5-10 degrees. Medially rotate the knee 45-55 degrees from the prone position.
Central ray Perpendicular to the IR, exiting the palpated patella. Collimate closely to the patellar area.
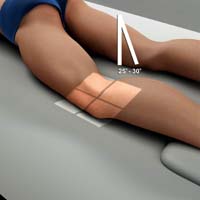
Patella PA Axial Oblique Kuchendorf Method
Purpose and Structures Shown Majority of the patella is seen free of superimposition by the femur. This projection is more comfortable for patients with an injured patella as it does not place any pressure on the patella.
Position of patient Prone position. Elevate the hip on the affected side by 2 or 3 inches. Place a sandbag under the ankle and foot. Adjust it so that the knee is slightly flexed (approximately 10 degrees) to relax the muscles.
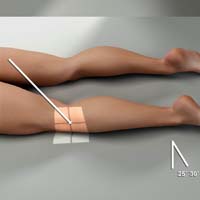
Position of part Center the IR to the patella. Laterally rotate the knee about 35-40 degrees from the prone position, which is more comfortable than the direct prone position. Place your index finger against the medial border of patella and press it laterally. Rest the knee on its anteromedial side to hold the patella in a position of lateral displacement.
Central ray Directed to the joint space between the patella and femoral condyles at an angle of 25-30 degrees caudad, entering the posterior surface of the patella.
Patella Tangential Projection Hughston Method
Purpose and Structures Shown Femoral condyles. This projection demonstrates subluxation of the patella and patellar fractures.
Position of patient Prone position with the foot resting on the table.
Position of part Place the IR under the patient’s knee. Slowly flex the affected knee so that the tibia and fibula form a 50 to 60 degrees angle from the table. Rest the foot against the collimator or support it in position.
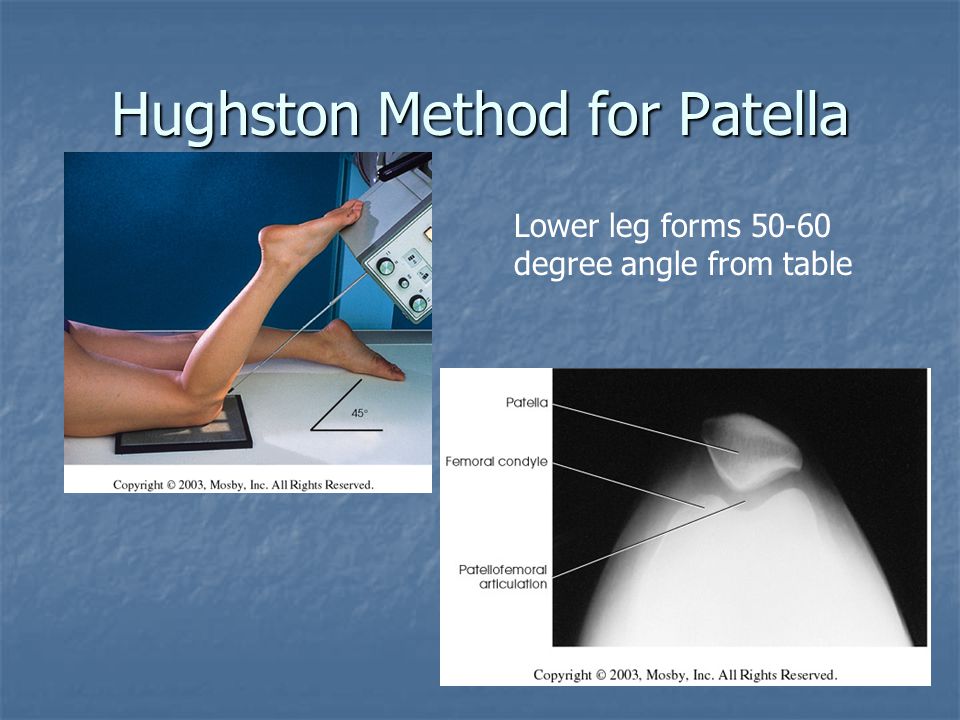
Central ray Angled 45 degrees cephalad and inferior and directed through the patellofemoral joint.
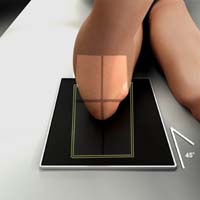
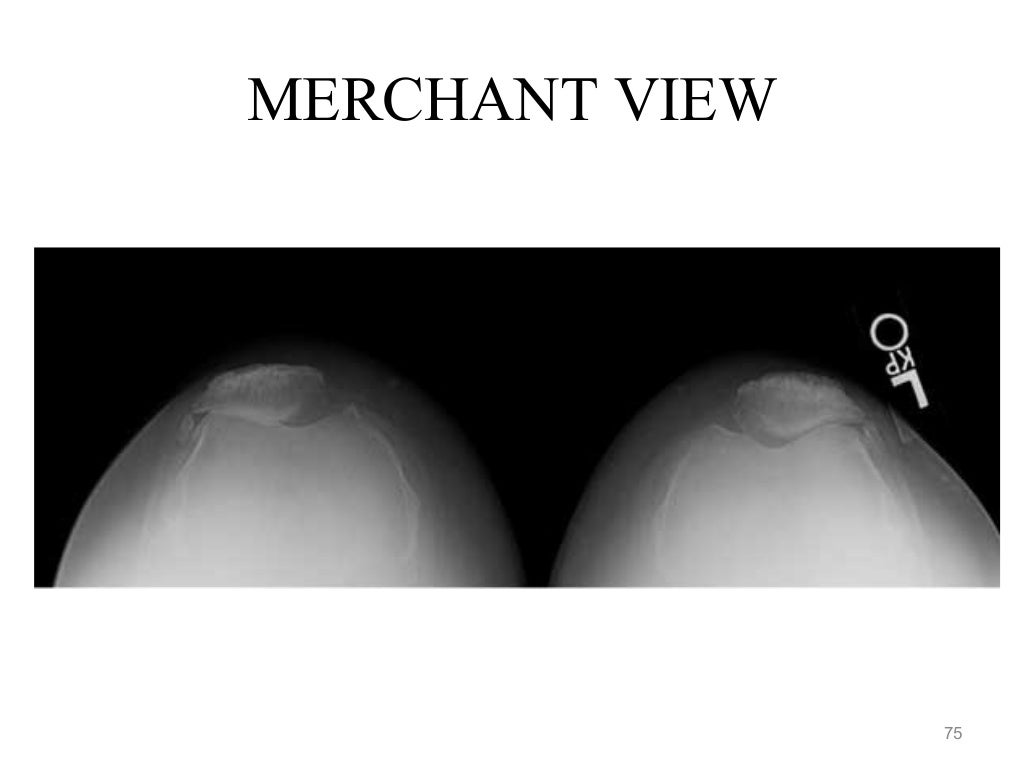
Patella Tangential Projection Merchant Method
Purpose and Structures Shown Axial projection of the patellae and patellofemoral joints, seen as slightly magnified images.
Position of patient Supine with both knees at the end of table. Support the knees and lower legs with an adjustable IR-holding device. Place pillows or a foam wedge under the patient’s head and back for comfort and to relax the quadriceps femoris.
Position of part Using the “axial viewer” device, raise the patient’s knees about 2 inches to place the femur parallel with the tabletop. Adjust the angle of knee flexion to 40-45 degrees. Strap both legs together at calf level to control leg rotation and allow the patient to relax. Place the IR perpendicular to the CR and resting on the patient’s shins about 1 foot distal to the patellae. Ensure that the patient is relaxed. Relaxation of quadriceps femoris is significant for accurate diagnosis. If not relaxed, a subluxed patella may be pulled back into intercondylar sulcus, which will result in a false normal appearance. Record the angle of knee flexion for reproducibility during follow-up examinations.
Central ray Perpendicular to the IR. The beam is directed caudal and inferior. With 45 degrees knee flexion, angle the CR 30 degrees caudal from the horizontal plane (60 degrees from the vertical) to achieve a 30 degrees CR-to-femur angle. CR enters midway between patellae at the level of the patellofemoral joint.

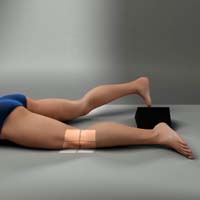
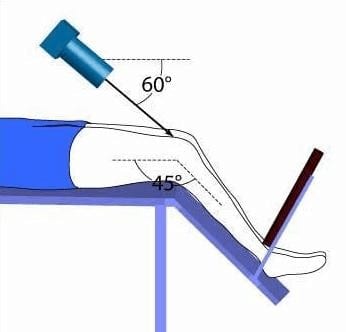
Patella Tangential Projection Settegast Method (Sunrise View)
Purpose and Structures Shown Provides information about the patella and patellofemoral articulation. It is an alternative method to obtain an axial image of the patella. A common technique is the inferosuperior projection. This projection involves acute flexion of the knee and should not be attempted until patellar fracture has been ruled out by other views.

Position of patient Supine or prone (prone is preferred because the knee can usually be flexed to a greater degree and immobilization is easier). In the prone position the IR is placed under the knee and the knee is flexed 115 degrees from the horizontal axis.


If the patient is seated on the radiographic table, the patient must hold the IR securely in place behind the knee. In the supine position, the patient’s knee is flexed 40-45 degrees with a knee support in place.

Position of part Flex the patient’s knee slowly as much as possible or until the patella is perpendicular to the IR (if the patient’s condition permits). With slow, even flexion, patient the will be able to tolerate the position, whereas quick, uneven flexion may cause excessive pain. Loop a long strip of bandage around the patient’s ankle or foot if desired. Have the patient grasp the ends of the string over the shoulder to hold the leg in position. Gently adjust the leg so that its long axis is vertical.
Central ray Perpendicular to the joint space between the patella and the femoral condyles when the joint is perpendicular. If not, degree of CR angulation depends on degree of flexion of the knee. The angulation typically will be 15 to 20 degrees from the lower leg. Close collimation is recommended.

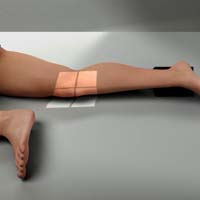
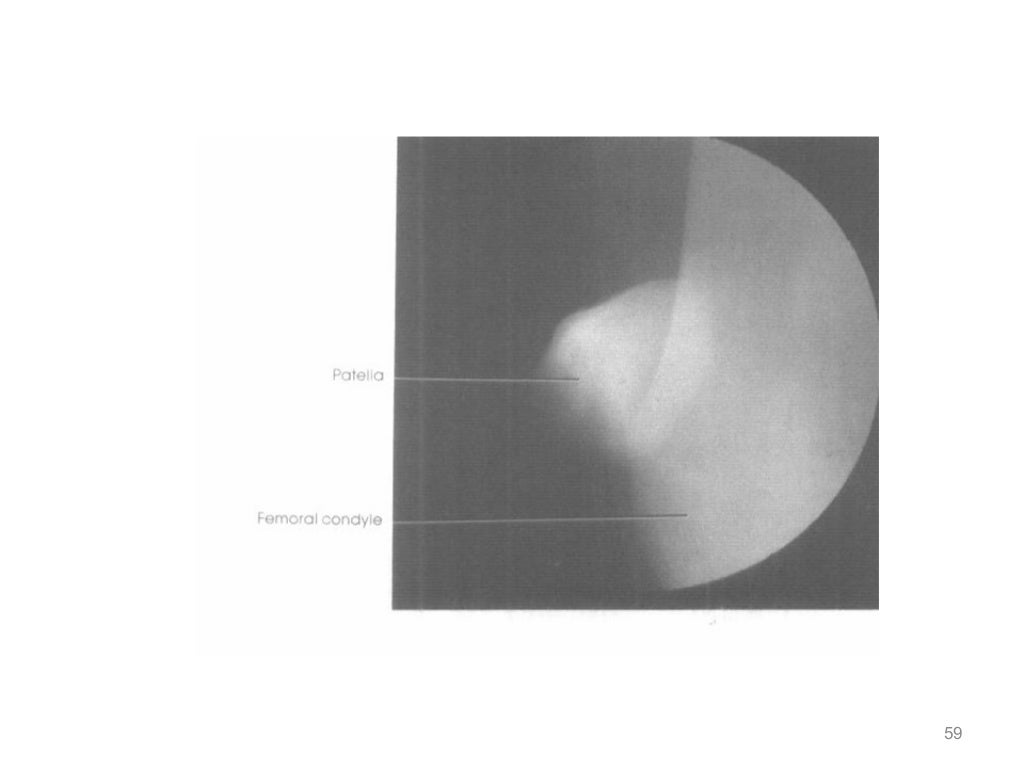
Patella Skyline Laurin View
Purpose and Structures Shown This is an inferosuperior axial projection of the patella which is visualized free from superimposition by any bony structure. The patellofemoral joint is clearly seen. The skyline projection demonstrates fractures on the lateral aspect of the patella that may be missed on other views.
Skyline Laurin Patella

Position of patient Semi-recumbent on the examination table with a pillow or cushion behind the back to enable the patient to maintain the position. The patient holds the IR superior to the patella in landscape orientation. The position of the patient should be as close to the end of the table as possible.

Position of part The knee is flexed 20-30 degrees. Ensure the patient’s feet are out of the primary beam.
Malpositioned Skyline Patella

Central ray The beam is directed cephalad and superior, 160 degrees from the vertical axis or 30 degrees from the horizontal axis. The X-rays pass inferior to superior through the patella. The tube will need to be below the level of the table.
Suggested Reading
Radiography of the leg and knee: An overview of anatomy and pathology
Radiographic positioning of the leg
Radiographic positioning of the knee in AP views
Radiographic positioning of the knee in PA views
Radiographic positioning of the knee in lateral views
RLKA
Read more about this and other subjects and get 2 Category A ARRT® CE Credits in the X-Ray CE Course “Radiography of the Leg, Knee, and Ankle”