Radiographic Positioning of the Knee Lateral Views
This article for Radiologic Technologists (X-Ray Techs) discusses radiographic positioning of the knee in lateral views.
Knee Lateral

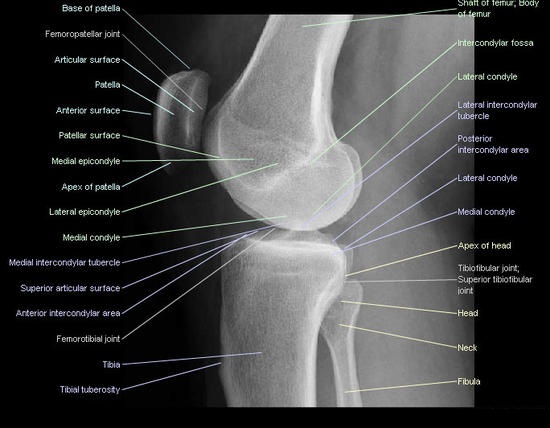
Purpose and Structures Shown To get a clear image of the patella in lateral profile. Structures seen are the distal end of the femur, patella, patellofemoral joint, proximal ends of the tibia and fibula, joint space between the tibia and femoral condyles, and adjacent soft tissue.
Position of patient For the rolled lateral position, the patient is placed in the lateral recumbent position with the affected side down. The affected knee is flexed 20 to 30 degrees. The pelvis should not be rotated. The opposite limb is extended and placed behind the knee being examined.
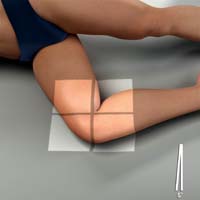
Position of part The detector is placed under the knee. The epicondyles are perpendicular to the IR. The patella is perpendicular to the plane of the IR. For new or unhealed patellar fractures, the knee should not be flexed more than 10 degrees (check with your medical director). Knee flexion of 20 to 30 degrees is otherwise preferred – this position relaxes the muscles and shows maximum volume of the joint cavity.

Central ray Directed 5 to 7 degrees cephalad to the knee joint 1 inch (2.5 cm) distal to the medial epicondyle. Slight angulation of the CR will prevent the joint space from being obscured by a magnified image of the medial femoral condyle. In the lateral recumbent position, the medial condyle will be slightly inferior to the lateral condyle.
Horizontal ray projection In trauma patients, a horizontal central ray lateral projection may be preferred to establish joint effusion or lipohemarthrosis (intra-articular fracture in which blood and fat escapes from the bone marrow into the joint). Also, this projection is ideal in trauma patients as it requires little to no movement by the patient. In this radiographic positioning of the knee, the affected knee is fully extended and the X-rays pass from lateral to medial.

Technical factors
- The lateral and medial condyles of the distal femur are superimposed on each other.
- True lateral position is when the poserior aspects of the medial and lateral femoral condyles are superimposed.
- The patellofemoral joint is open and projected free.
- The femorotibial joint space is open.
- There is slight superimposition of the fibular head with the tibia.
- The patella is in lateral profile. The peripatellar fat pads are adjacent to each other.
- The medial and lateral condyles can be differentiated by the presence of the medial adductor tubercle on the lateral condylopatellar sulcus, respectively.
- Oblique images can be obtained by external or internal rotation of the knee from neutral supine position.
Knee in true lateral position
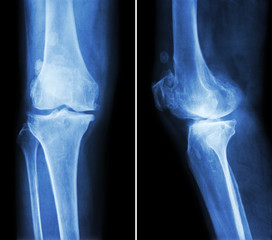
Malpositioned knee in rolled lateral projection

Image source : wikiradiography.net
Suggested Reading
Radiography of the leg and knee: An overview of anatomy and pathology
Radiographic positioning of the leg
Radiographic positioning of the knee in AP views
Radiographic positioning of the knee in PA views
Radiographic positioning of the knee in patella views
RLKA
Read more about this and other subjects and get 2 Category A ARRT® CE Credits in the X-Ray CE Course “Radiography of the Leg, Knee, and Ankle”