Osteogenesis Imperfecta or Abuse: Can You Tell the Difference?
The human skeleton can be affected by a number of developmental disorders and genetic abnormalities. One of the most common developmental disorders of the skeleton is a spectrum of inherited conditions called osteogenesis imperfecta (OI) or brittle bone disease. Individuals with this disorder have fragile bones that are prone to fractures. There are various osteogenesis imperfecta types that result from mutations or genetic defects.
X-ray technologists often encounter patients with OI when they present for radiographic imaging of fractures. However, it can be difficult to tell the difference between OI (especially the milder osteogenesis imperfecta types) and non-accidental injuries. Let’s take a look at the causes, types, and symptoms of this condition, the role of DXA in diagnosis, and how to tell the difference between OI and abuse.
Osteogenesis Imperfecta Causes
OI is a generalized connective tissue disorder. It occurs because of genetic abnormalities that inhibit the normal production of collagen type I, a protein which forms the underlying structural framework of bone. The disease can vary in severity from mild (relatively asymptomatic) to severe (resulting in stillbirth or early death). In the majority of patients with osteogenesis imperfecta, however, low bone mass (some degree of osteopenia) is present, resulting in multiple fractures and skeletal deformities.
Osteogenesis Imperfecta Types
Osteogenesis imperfecta is categorized into four types based on how severe and longstanding the patient’s symptoms are.
Type I
Type I OI is the most commonly occurring type and also the least severe version of the disease. Patients with type I OI typically suffer a few fractures.
Type IV
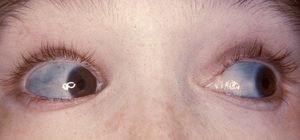
In terms of severity, type IV OI is next (it is named type IV as it was discovered after the first three types). Patients with type IV OI usually have mild to moderate deformities and may also exhibit other symptoms such as hearing loss and dental problems. Sometimes people with type IV OI exhibit blue sclerae and have a gray, blue, or purple discoloration of the white portion of the eye.
Type III
The next among osteogenesis imperfecta types is Type III which is a severe form of OI. Patients with this form of the disease have a relatively high frequency of fractures and exhibit a short stature. They may also suffer from dental problems and hearing loss.
Type II
The most severe among osteogenesis imperfecta types is II. Patients with this form of the disease usually suffer several fractures and have severe deformities with a short life expectancy.
Osteogenesis Imperfecta Symptoms
The clinical presentation of osteogenesis imperfecta varies greatly depending on severity. Some babies with OI suffer multiple fractures while still in their mother’s womb and are stillborn because of an inability to breathe. At the other end of the spectrum, children with mild osteogenesis imperfecta types suffer very few fractures when they are older, similar to osteoporosis.
Of particular interest is a scenario where a child suffers multiple fractures in the early years of life but does not have the telltale signs of the disease such as blue sclerae. Because OI remains undiagnosed in such children, their parents are sometimes accused of child abuse. A similar confusion may occur in victims of domestic violence.
A definitive diagnosis of OI can be made by tissue analysis, but this test is not widely available and is difficult to perform and expensive. In most cases, the frequency of fractures decreases as the child grows older. Fractures typically stop occurring at puberty. However, as adults, these people tend to have a short stature and considerable deformities. Nonetheless, with proper support in the home and work environment, they can usually function well.

It has been noted that female patients with osteogenesis imperfecta types I to IV often begin to fracture again when they reach menopause. Because OI can be treated and fracture prevention measures can be instituted, it is important for the disease to be identified early. This also allows relatives of a patient to be tested for the disease. Healthcare professionals such as pediatricians, emergency room physicians, and orthopedists who see children and adults with unprovoked fractures should remain aware of OI as a possible cause, especially in patients and families with a history of recurrent fractures.
Role of DXA in OI Diagnosis
Skin biopsy is the definitive method of diagnosis for osteogenesis imperfecta types I through IV. This test can detect abnormal collage type I structure or synthesis in upto 90 percent of patients. However, it is not 100 percent sensitive and some patients may have OI and a normal skin biopsy. Also, test results can take 3 months to be available. Can DXA scans diagnose OI?
Studies show that DEXA of the spine has a more than 90 percent sensitivity for OI. DXA of the whole body has an 80 to 100 percent specificity for OI. Therefore, DXA has a role in the evaluation of osteogenesis imperfecta types. However, it should be kept in mind that some patients with OI can have normal DEXA results and some patients without the disease can have low DEXA results.
How to Tell the Difference Between OI and Non-Accidental Injuries?
For the milder osteogenesis imperfecta types, it can be difficult to distinguish the disease from non-accidental injuries (abuse).
Features of history suspicious for abuse:
- Fractures without significant trauma
- Delayed reporting
- Inconsistent history
- No repeat fractures in protective environment
- Concomitant head injuries and unusual skin injuries
Features of fracture patterns suspicious or pathognomic (characteristic) for abuse:
- Multiple fractures at different stages of healing
- Bucket handle or metaphyseal corner
- Posterior rib fractures near the costovertebral junction
- Lower extremity fracture in non-weightbearing child
- Acute bilateral extremity fractures
- Acute epiphyseal fracture in very young child
Features of history suspicious for osteogenesis imperfecta:
- Frequent fractures with minimal trauma
- Easy bruisability
- Blue sclerae
- Lax joints
- Soft, discolored teeth
- Abnormal head shape
- Short stature
- Excessive sweating and heat intolerance
- Family history of OI or above features
Clinical findings suspicious for OI:
- Osteopenia on DXA
- Bone deformities
- Wormian bones (mosaic pattern of sutural bones absent in normal skulls)
Osteopetrosis: How Is It Different from OI?
In addition to osteogenesis imperfecta types I to IV, another set of rare developmental disorders affecting the skeleton are sclerosing bone diseases. Osteopetrosis, also known as marble bone disease, is one such condition which is associated with an excessive accumulation of bone, making it essentially the reverse of osteoporosis.
Whereas in osteoporosis the osteoclasts are overactive, in osteopetrosis a genetic defect leads to impairment in the osteoclasts such that they are underactive and unable to properly perform bone resorption. The resultant accumulation of very dense bone leads to abnormal skeletal development. This bone, although very dense, is also very brittle and can easily fracture. In addition, this excessive bone compresses upon nerves and causes neurological symptoms, which is why patients who have osteopetrosis may develop blindness or deafness. The excess bone can “crowd out” red cells in the bone marrow, leading to anemia. Fibrous dysplasia is a condition where, similarly, an excessive amount of connective tissue is produced by cells that form bone.
X-ray CE
We offer a range of online courses for X-ray CE. Our course Radiography of the Upper Extremities is worth 24 CE credits. It allows X-ray techs to complete biannual ARRT® requirements with one easy and convenient e-course.
Read more about this and other subjects and get 24 Category A ARRT® CE Credits in the X-Ray CE Course “Radiographic Bone Densitometry”DXA
Here is more information about radiologic technologist continuing education.