DXA Results Interpretation: A Quick Guide for X-ray Techs
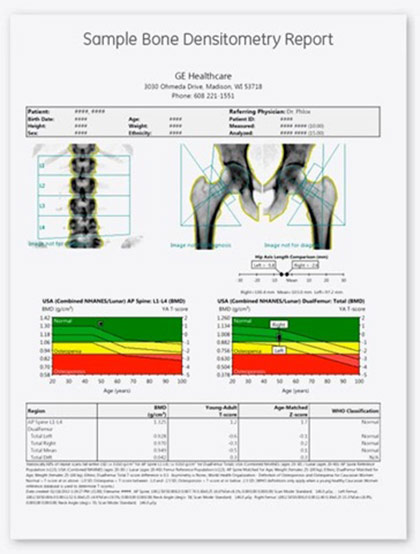
DXA is the most commonly used machine for BMD measurement. It is more common than other modalities such as QCT in osteoporotic patients. X-ray techs need at least a basic knowledge of DXA results interpretation. DXA results are expressed by two numbers known as T-score and Z-score.
T-Score
The T-score is an indication of the amount of bone an individual has compared to peak bone mass in a young adult of the same gender. When the T-score is more than -1, it is indicative of normal density. When the T-score is less than -1 but more than -2.5, it is called osteopenia. When the T-score is under -2.5, it is called osteoporosis. Therefore, a person’s T-score can be used to estimate their likelihood of suffering a fracture.
According to WHO guidelines for DXA results interpretation, “established osteoporosis” in white women is a T-score that is greater than two and a half standard deviations under the reference average in an adult (young) female; however, the organization does not have sufficient data to create similar definitions for men and other ethnic groups. Therefore, it should be noted that the database which is referenced for T-scores is that of a white female and is not adjusted for race or gender.
Z-score
Z-score is a number that shows the amount of bone an individual has compared to others of the same gender, age, and body size. An unusually high or low Z-score warrants further investigation during DXA results interpretation. A Z-score worse than -2.0 is considered below expectation for the individual’s age. A Z-score that is more than 2.0 is considered as expected for age. Low Z-scores may suggest an increased likelihood of secondary osteoporosis, although such an index of suspicion has not been validated by clinical trials. BMD reporting with Z-scores is preferred in children, premenopausal women, and males younger than age 50.
Changes in DXA Results
It is important to be aware during DXA results interpretation that minor changes are not clinically relevant. Small changes in these scores (T or Z) between two successive scans can occur due to positioning. BMD should ideally be measured on the same equipment each time or on equipment made by the same manufacturer to avoid errors. Conversions of BMD from one manufacturer to another or differences between two machines can introduce errors that are large enough to render the test ineffective.
Diagnostic Caveats in DXA Results Interpretation
In addition, clinicians and radiologic technologists should be aware of certain diagnostic caveats during DXA results interpretation. A T-score of less than -2.5 does not necessarily indicate osteoporosis (it could be osteomalacia, for example). Also, even though a T-score of -1.9 is not classified as osteoporosis, in the presence of a vertebral fracture caused by minimal or no trauma, a clinical diagnosis of osteoporosis should be considered. Finally, a low T-score does not identify the cause of osteoporosis and further medical evaluation should be considered to address possible treatable causes of the disease.
DXA Results Interpretation in Children
DXA measurements in children deserve special consideration, as does DXA results interpretation. This is because T-score compares the bone mineral density of a child to reference data obtained in adults. During childhood, maximum bone mass has not yet been attained, and the T-score therefore underestimates BMD in children. In other words, calculating T-score in children can lead to overestimation of bone deficit and over-diagnosis of osteopenia or osteoporosis. For this reason, Z-score is a better method of estimating BMD in children because it compares the child’s score to reference values for individuals of the same age and gender.

Bone Size and Interpretation of DXA Results
Another confounding factor in DXA results interpretation is bone size. In general, DXA tends to overestimate BMD in taller individuals and underestimate BMD in people of shorter stature. This error occurs because DXA machines measure the reduction in intensity of the beam by bones and divide this by the area of the body part being scanned. Thus, DXA measures areal density in grams/cm2 and not true volumetric bone density in grams/cm3. This has clinical relevance because people of other ethnicities have a different body habitus than white women who are the reference group for the T-score-based diagnosis of osteoporosis.
X-ray Continuing Education
We offer CE courses to complete ARRT® requirements. Please visit our shop and purchase one of our online courses. You can conveniently read the material in the comfort of your home. Once you pass the post-exam, you will immediately receive a certificate of completion. Our bone densitometry course is ideal for DXA operators, but also appropriate for general radiographers. It is worth 23 CEUs.
Read more about this and other subjects and get 24 Category A ARRT® CE Credits in the X-Ray CE Course “Radiographic Bone Densitometry”DXA
Here is details about ce credits for x ray techs