Radiographic Positioning of the Zygomatic Arch
The zygomatic arch (cheekbone) is composed of the temporal bone’s zygomatic process and the zygomatic bone’s temporal process, which is joined by an oblique suture, namely zygomaticotemporal suture. Fractures of the zygoma region can occur with head trauma. In fact, the zygomatic arch is one of the most commonly fractured facial bones, typically following altercations in which the patient is punched in the face. Most zygomatic fractures are followed by a sensory abnormality, either hypoesthesia or anesthesia, in one or more branches of the infraorbital nerve. Radiographic confirmation of zygomatic arch fractures allows early stabilization with better anatomic function and cosmetic results.
Anatomy of the Zygoma
The skull is made of several bones that are held together at sutures by connective tissue called sutural ligaments. The bones of the skull can be categorized into the cranium and the face (see our article on radiographic positioning of the skull for the major projections used to image the cranial bones). The cranium consists of:

- Frontal bone
- A pair of parietal bones
- Occipital bone
- A pair of temporal bones
- Sphenoid bone
- Ethmoid bone
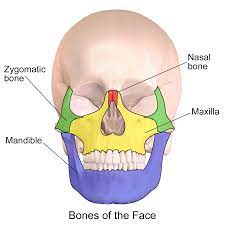
The facial bones include:
- A pair of zygomatic bones
- A pair of maxillae
- A pair of nasal bones
- A pair of lacrimal bones
- Vomer
- A pair of palatine bones
- A pair of inferior conchae
- Mandible
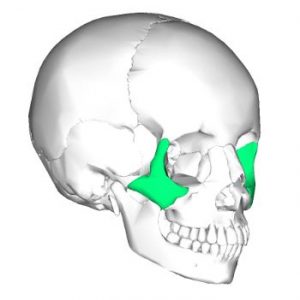
The facial bones form the structure of the face. The zygomatic bones (also referred to as the malar bones) are a pair of quadrilateral-shaped bones responsible for the prominence of the cheeks. The term “zygomatic” comes from the Greek word “zygoma” which means “yoke.” The zygomatic bone on each side is located below and lateral to the eye socket. It borders the frontal bone lateral to the orbit and the sphenoid and maxilla medially.
Anatomical Structure of the Zygomatic Bone
The zygomatic bone has four projections, which give it the characteristic quadrilateral (diamond) shape. The superior projection connects with the frontal bone. Medially, it forms the lateral portion of the infraorbital rim. Posteriorly, it forms the anterior portion of the zygomatic arch. Inferiorly, it connects to the alveolus of the maxilla. The zygomatic bone is responsible for the malar prominence, an important aesthetic landmark in facial architecture. The zygomatic arch provides width to a person’s face and figures prominently in the oblique facial profile. Besides its aesthetic significance, the zygomatic-maxillary region plays an important functional role. It provides stability and support to the midface and protection to the orbit.
Surfaces of the Zygomatic Bone
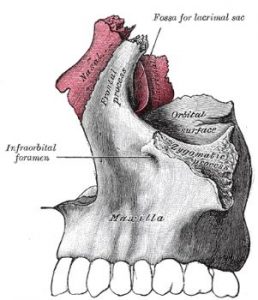
There are three surfaces to the zygomatic bone: malar, posteromedial, and orbital. ⦁ The malar (facial or cheekbone) surface is exposed to the elements. It is smooth and convex, with a tiny aperture known as the zygomaticofacial foramen. The zygomaticofacial nerve, artery, and vein pass via this foramen between the orbit and the face. The lateral surface also acts as an attachment point for the zygomaticus major and zygomaticus minor muscles on the anterior half and the zygomaticus minor muscle on the posterior half. ⦁ The temporal (posteromedial) surface is concave with a rough triangular area medially for articulation with the maxilla and a smooth concave surface laterally that forms the anterior boundary of the temporal fossa and the lower part of the infrate temporal fossa. The posteromedial surface extends over the medial side of the temporal process, forming a portion of the infrate temporal fossa’s lateral wall. The zygomaticotemporal foramen, located near the base of the frontal process, transports the zygomaticotemporal nerve from the orbit to the temporal fossa. ⦁ The orbital surface is concave and smooth. It constitutes the anterolateral region of the floor and the anterior part of the lateral wall and confronts the orbit. It has the zygomatico-orbital foramen, which is a portal to the bony canal located within the zygomatic bone. This canal divides into the zygomaticofacial and zygomaticotemporal canals, which open on the respective zygomatic bone surfaces. The former carries the zygomaticofacial nerve and vessels, whilst the latter carries the zygomaticotemporal nerve and vessels.
Processes of the Zygomatic Bone
The zygomatic bone on each side is diamond-shaped with three processes that articulate with the frontal, temporal, and maxillary bones. Each process forms an important structural component of the skull. ⦁ The frontal process arises from the zygomatic bone’s top edge. It is superiorly oriented and includes the orbit’s lateral contour. The zygomatic frontal suture connects it to the zygomatic process of the frontal bone superiorly, while the sphenozygomatic suture connects it to the larger wing of the sphenoid bone posteriorly. Whitnall’s tubercle is a bony tubercle on the orbital surface of the frontal process that acts as an attachment place for the lateral palpebral ligament, suspensory ligament of the eye, and the aponeurosis of the levator palpebrae superioris muscle. ⦁ The temporal process arises from the zygomatic bone’s bottom half. It is positioned posteriorly and somewhat superiorly to the temporal bone. The temporal process’s terminal tip is oblique and jagged, and it articulates with the temporal bone’s zygomatic process, which forms the zygomatic arch. ⦁ The maxillary process develops from the zygomatic bone’s anterior superior angle. It extends anteriorly, encompassing the orbit’s inferolateral edge. This process’s inferior margin is involved in the junction with the maxilla. It is continuous with the orbital surface of the bone posteriorly.
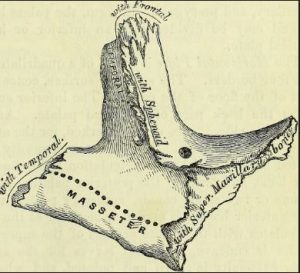
Borders of the Zygomatic Bone
The zygomatic bone is divided into five sections: ⦁ The anterosuperior (orbital) border is smooth and concave. It is the zygomatic bone’s boundary between the lateral and orbital surfaces. ⦁ The zygomaticomaxillary suture is articulated on the anteroinferior (maxillary) boundary. It also acts as a place for the levator labii superioris muscle to connect. ⦁ The posterosuperior (temporal) border is continuous with the zygomatic arch’s superior border and the frontal process’s posterior border. It acts as a site of attachment for the temporal fascia. ⦁ The posteroinferior border is rough and acts as the masseter muscle attachment place. ⦁ The posteromedial border is serrated and articulates superiorly with the larger wing of the sphenoid bone and inferiorly with the orbital surface of the maxilla through the sphenozygomatic suture. There is a little free surface of the posteromedial edge between the articular surfaces that forms the lateral boundary of the inferior orbital fissure.
Articulations of the Zygomatic Bone
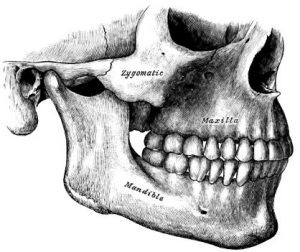
The zygomatic bone articulates with four bones – the frontal, temporal, sphenoid (greater wing), and maxilla.
Development of the Zygomatic Bone
The zygomatic bones ossify from three points, two in orbital area and one in the malar area. These ossification points appear at about the eighth week of gestation and fuse at around the fifth month. After birth, the zygomatic bone may sometimes be divided horizontally by a suture into a larger upper portion and a smaller lower portion.
Facial Bone Trauma
Fractures of the skull are common in adults, but occur less often in young children. The skull bones of an infant are more resilient compared to an adult because they are separated by fibrous sutural ligaments. In the adult skull, the bones are brittle due to their composition and structure. In addition, sutural ligaments become ossified as a person ages. The type of skull bone fracture largely depends on the location and intensity of the trauma as well as the age of the patient. The adult skull can be compared to an eggshell with limited strength and resilience beyond which it breaks. In a young child, the skull can be compared to a table tennis ball where a blow creates a depression without causing a break in the bone. The developing facial bones of a child are more pliant than that of adults. Therefore, most facial bone fractures in children are greenstick or incomplete. In adults, however, most facial fractures are open fractures with a risk of infection and need for antibiotic therapy. Falls, fist fights, and motor vehicle accidents are the most common causes of facial fractures. Signs of fracture of the facial bones include deformity, ocular/orbital displacement, abnormal movements accompanied by cracking or rattling sounds, and malocclusion of the teeth. The most common facial fractures involve the nasal bones, followed by the zygomatic bones, and then the mandible. Fractures of the zygoma can occur with a blow to the lateral face. This type of trauma can result in an isolated fracture, such as from the impact of a clenched fist. However, it can also occur in conjunction with other fractures of the face, usually as a result of MVAs or other high-impact injuries. Moderate force can cause slightly displaced or non-displaced fractures at the suture lines. More forceful trauma usually results in displacement of the zygoma inferiorly, medially, or posteriorly.
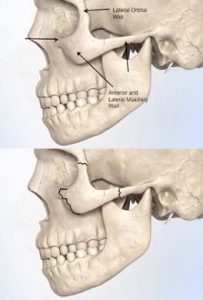
Top: Schematic Structure of the Zygomatic Area. Bottom: Areas of the Zygomatic Bone that are Commonly Fractured (© Osborne Head & Neck Institute).
Zygomatic Bone Fractures Simple Fractures
Simple zygomatic arch (orbitozygomatic) fractures are usually the result of a blow to the lateral face, for example, during a fist fight or from an object such as a baseball. They may also occur as a result of car crashes. They are less frequent than tripod fractures.
Tripod Fracture:
A tripod fracture is a combination of three fractures that often include the zygomatic arch, frontozygomatic and maxillo zygomatic sutures, and the zygomatic arch. A free-floating zygomatic bone is the outcome of this sort of triple fracture. This form of comminuted fracture, which results in suture line dissociation, is most commonly seen in high-impact motor vehicle accidents or explosions
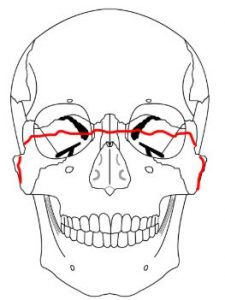
Le Fort III Fracture:
This is a transverse fracture of the midface. It is also called craniofacial dissociation. It involves the pterygoid plate and zygomatic arch.
Radiographic Positioning of the Zygoma
Patients with suspected facial trauma and/or zygomatic fractures are evaluated primarily with craniofacial X-rays or CT scans. Several different radiographic views are useful to observe specific parts of the skull. The most common views that enable visualization of the zygomatic area are:
- Occipitomental (OM) or Water’s View
- Submentovertex (SMV) View
- Facial or Caldwell’s View
Occipitomental (OM) or Water’s View:
This is an angled PA radiograph of the skull taken with the patient erect and facing an upright IR. The head is tilted back slightly so that the patient is gazing upwards. The chin is raised until the mentomandibular line is perpendicular to the IR and the orbitomeatal line is at an angle of 37 degrees to the IR. The central ray of the X-ray beam exits at the acanthion. This projection displays the orbital rim, floor of the orbit, maxillary sinuses, nasal septum, nasal bones, and zygomatic bones.

https://www.youtube.com/watch?v=D7WHs2wv2GQ Video Credit : Dentistry Madeeasy
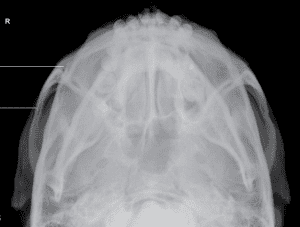
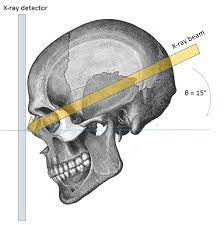
Submentovertex (SMV) View:
This is a radiograph taken with the patient’s chin raised and neck fully extended. Cervical spine injuries and fractures must be ruled out prior to attempting this projection in trauma patients. The midsagittal plane (MSP) of the body is at a right angle to the IR. The infraorbitomeatal line (IOML) must be parallel to the Image Receptor (IR). The X-ray beam passes through the underside of the chin and exits are the vertex of the skull. The beam is directed perpendicular to the acanthomeatal line. This projection is used in combination with other views to maximize the visualization of skull structures. The SMV projection should show both zygomatic arches with a single exposure.

Positioning of Submentovertex view
Video Credit : Chase Smith
Caldwell’s View:
Also called the occipitofrontal projection, this is an angled radiograph of the skull in which the plate is angled at 20 degrees to the orbitomeatal line. The patient is seated in front of a vertical detector with the forehead and nose pressed against the IR. The orbitomeatal line is at a right angle to the IR. The structures visualized on this projection include the paranasal sinuses (frontal and ethmoidal), orbits, orbital rims, medial orbital walls, zygomatic bones, nasal bones, nasal septum, and mandible.
In patients with suspected facial fractures, a basic facial series imaging workup is usually requested, consisting of three or four films. Of the various projections, Water’s view is preferred because it demonstrates all major facial structures more clearly than other views. With advancements in medical technology, high-resolution computerized tomography (CT) scans have, for the most part, become the imaging modality of choice in patients with facial trauma. Compared to plain film radiography, CT scans more clearly demonstrate the complex bony anatomy of the face and the intricacy of injuries resulting from facial trauma. Get latest information about radiologic technologist ce credits and arrt® continuing education credits here.